Categories
Change Password!
Reset Password!


Bempedoic acid (BA) is an orally bioavailable prodrug and suppressor of adenosine triphosphate-citrate lyase (ACL), exerting anti-hyperlipidemic effects.
Bempedoic acid (BA) is an orally bioavailable prodrug and suppressor of adenosine triphosphate-citrate lyase (ACL), exerting anti-hyperlipidemic effects.[1,2] This lipid-lowering agent plays a key role in treating those with raised levels of low-density lipoprotein cholesterol (LDL-C) levels. [1]
It was approved by the FDA on 21 Feb 2020 as an adjunct to maximally tolerated statin therapy for minimizing LDL-C, specifically in those afflicted by atherosclerotic cardiovascular disease (ASCVD) and heterozygous familial hypercholesterolemia (HeFH). It is also a viable substitute for those intolerant to statins. [1,3]
Pharmacological class: ACL inhibitor
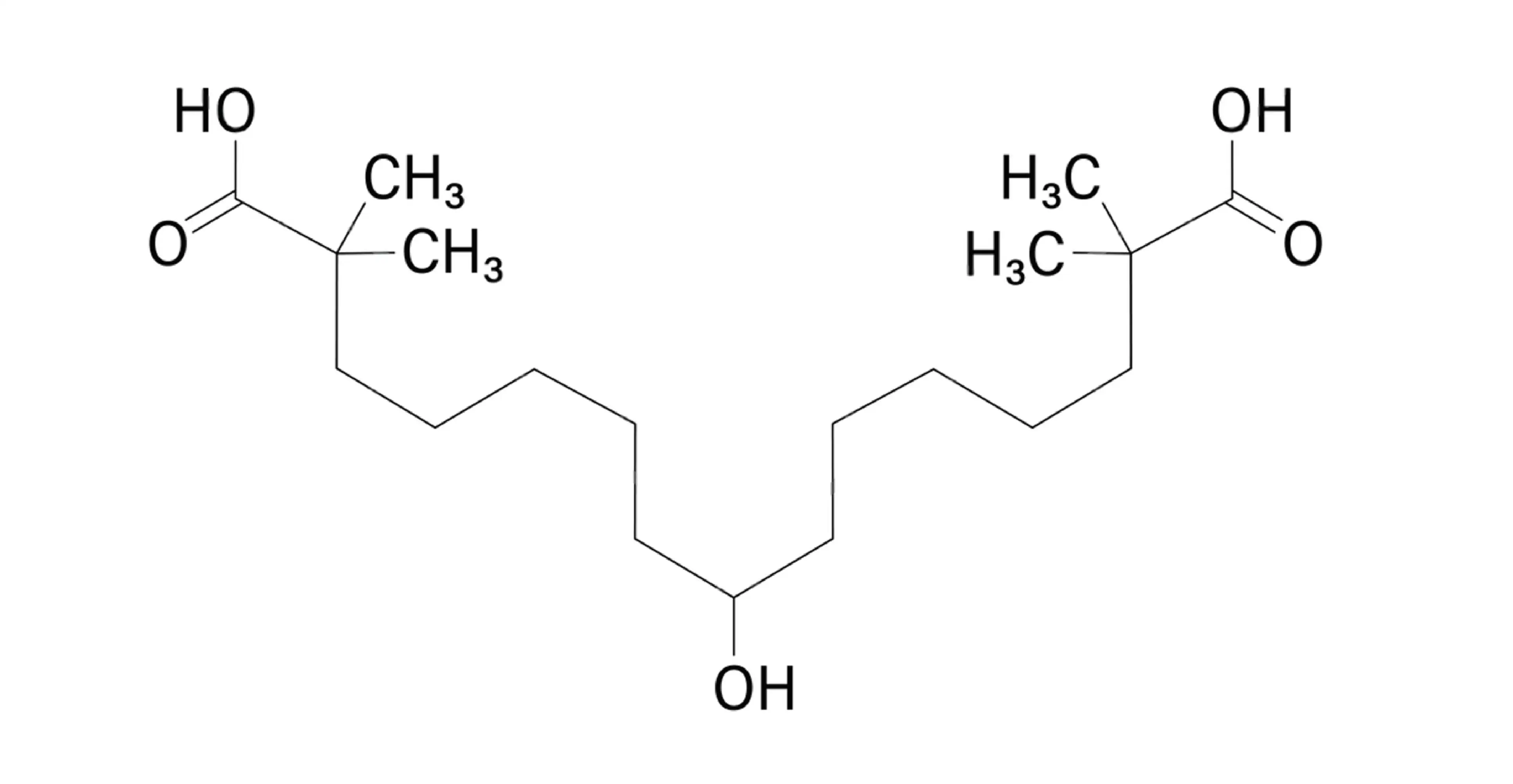
BA (C19H36O5; also known as 8-hydroxy-2,2,14,14-tetramethylpentadecanedioic acid) is indicated to lower the chances of myocardial infarction and coronary revascularization in adults with established cardiovascular disease or those at high risk for a cardiovascular event who are unable to tolerate the suggested statin therapy. It is also authorized as an adjunct to diet, with or without additional LDL-C lowering therapies, to minimize LDL-C levels in adults suffering from primary hyperlipidemia, including HeFH. [1,3,4]
LDL-C is primarily generated in the liver and travels via the bloodstream. When the blood levels of LDL become excessive, the surplus can deposit within blood vessel walls—including coronary arteries—raising the risk of cardiovascular events. BA is a prodrug that requires hepatic activation. It is converted to its active form, ETC-1002-CoA. The enzyme very-long-chain acyl-CoA synthetase-1 (ACSVL1), expressed primarily in the liver, plays a key role in this conversion. ETC-1002-CoA then suppresses ATP-citrate lyase, a fundamental enzyme implicated in the synthesis of cholesterol.
This inhibition leads to the upregulation of LDL receptors in the liver, boosting the uptake and clearance of LDL-C from the bloodstream. Through these mechanisms, BA successfully lowers circulating LDL-C levels, which are known to contribute to vascular damage and atherosclerosis. Additionally, in rodent models, ETC-1002 activates AMP-activated protein kinase (AMPK), resulting in further inhibition of cholesterol synthesis via suppression of HMG-CoA reductase activity. But, the clinical relevance of this effect in humans remains uncertain. [3]
Administer 180 mg by mouth once daily, regardless of food intake. [4]
Absorption
BA is quickly absorbed in the small intestine. Following administration of a 180 mg tablet, peak plasma concentration (Tmax) is typically reached in approximately 3.5 hours.
Volume of distribution
BA's apparent volume of distribution is about 18L.
Protein binding
The plasma protein binding of BA and its metabolites is about 99%.
Metabolism
BA is mainly metabolized into two primary compounds: ETC-1002-CoA and ESP15228. The drug undergoes elimination largely through conversion to its acyl glucuronide form. In vitro data suggest that BA can be reversibly transformed into the active metabolite ESP15228. Both ETC-1002-CoA and ESP15228 are further processed into inactive glucuronide conjugates, primarily through the action of the enzyme UGT2B7.
Route of elimination
Conjugated forms of BA are primarily excreted through the urine (approximately 70%) and to a lesser extent via the feces (around 30%). Only about 5% of the delivered dose is recovered as an unchanged drug in both urine and feces combined.
Half-life
The elimination half-life typically falls within a range of 15 to 24 hours. According to prescribing data, the average half-life is approximately 21 ± 11 hours.
Clearance
At steady state, the apparent clearance has been estimated at 11.2 mL/min based on clinical trial findings. [3]
Due to the heightened risk of muscle-linked adverse effects:
The most common adverse reactions (incidence ≥ 2%) include:
An interim analysis of the Italian cohort from the MILOS study investigated the real-world effectiveness and safety of BA or a fixed-dose combination of BA with ezetimibe (BA+EZE FDC) over 8 weeks in patients with hypercholesterolemia or mixed dyslipidemia. Among 855 patients with complete LDL-C data, treatment with BA or BA+EZE led to a mean LDL-C reduction of 22.6%, and the proportion achieving LDL-C goals rose from 7.1% to 37.2%, especially among very high cardiovascular risk patients. No novel safety concerns were reported. These findings support BA/BA+EZE as effective LDL-C lowering therapies in clinical practice. [5]
A pooled analysis of two 52-week phase 3 trials investigated BA's effectiveness and safety as an add-on lipid-lowering therapy in people suffering from HeFH and/or ASCVD already receiving maximally tolerated statin therapy. Out of 3,009 volunteers, 217 had HeFH (BA: 146; placebo: 71). At week 12, BA markedly reduced LDL-C levels when compared to placebo in both groups:
BA also led to prominent reductions in other lipid parameters and high-sensitivity C-reactive protein (hs-CRP), irrespective of HeFH status. Among HeFH patients treated with BA, 32% attained LDL-C <100 mg/dL at week 12, and 27% sustained this goal through week 52—a notable achievement given the high baseline LDL-C (mean: 172.8 mg/dL). The safety profile was consistent across all subgroups, with treatment-emergent adverse events occurring in nearly 75% of subjects in both treatment and placebo arms. No new safety concerns were observed in HeFH patients despite their more intensive lipid-lowering regimens. Thus, BA offers a clinically meaningful LDL-C reduction and is generally well-tolerated, making it a valuable adjunct for HeFH sufferers who remain above LDL-C targets despite statin-based therapy. [6]
A 78-week open-label extension (OLE) study investigated BA's long-term safety and efficacy following the 52-week CLEAR Harmony phase 3 trial in patients with ASCVD and/or HeFH. Of the 1,462 volunteers enrolled, 970 continued BA (up to 130 weeks total), while 492 switched from placebo to BA (for up to 78 weeks).
Overall, BA was generally well-tolerated and illustrated sustained lipid-lowering efficacy with up to 2.5 years of continuous treatment. [7]
1. Chandramahanti S, Patel P, Farzam K. Bempedoic Acid. [Updated 2024 Feb 28]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK594232/
Bookshelf ID: NBK594232, PMID: 37603623.
2. Bempedoic acid. PubChem [CID:10472693]. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Bempedoic-Acid
3. Bempedoic acid. Drug Bank [ID: DB11936]. Available from: https://go.drugbank.com/drugs/DB11936
4. NEXLETOL (bempedoic acid) tablets. FDA Label. Available from: www.accessdata.fda.gov/drugsatfda_docs/label/2020/211616s000lbl.pdf
5. Averna M, Gouni–Berthold I, Jukema J, Van Lennep JR, Ray K, Koskinas K et al. EVALUATING DYSLIPIDAEMIA TREATMENT WITH BEMPEDOIC ACID AND EZETIMIBE OVER 8 WEEKS IN THE ITALIAN COHORT OF THE MILOS OBSERVATIONAL STUDY. European Heart Journal Supplements. 2025 May;27(Supplement_5):suaf076-356.
6. Duell PB, Banach M, Catapano AL, Laufs U, Mancini GJ, Ray KK et al. Efficacy and safety of bempedoic acid in patients with heterozygous familial hypercholesterolemia: analysis of pooled patient-level data from phase 3 clinical trials. Journal of Clinical Lipidology. 2024 Mar 1;18(2):e153-65.
7. Ballantyne CM, Banach M, Bays HE, Catapano AL, Laufs U, Stroes ESG et al. Long-Term Safety and Efficacy of Bempedoic Acid in Patients With Atherosclerotic Cardiovascular Disease and/or Heterozygous Familial Hypercholesterolemia (from the CLEAR Harmony Open-Label Extension Study). The American Journal of Cardiology. 2022 Jul 1;174:1-11.













Comments (0)