Categories
Change Password!
Reset Password!


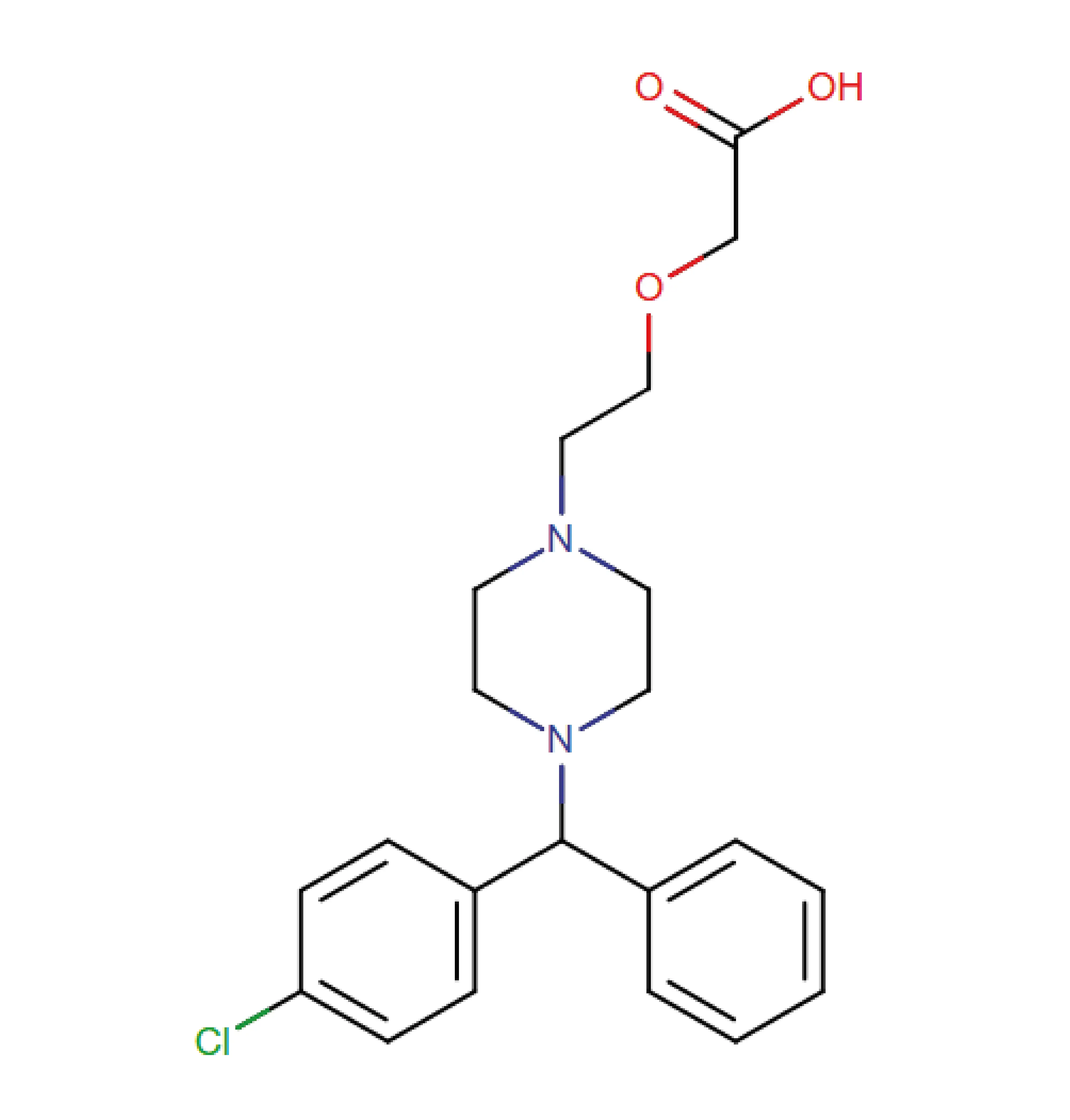
Cetirizine is a second-generation antihistamine widely recognized for its efficacy in managing various allergic conditions while minimizing central nervous system (CNS) side effects.
Cetirizine is a second-generation antihistamine widely recognized for its efficacy in managing various allergic conditions while minimizing central nervous system (CNS) side effects. Initially approved by the U.S. Food and Drug Administration (FDA) in 1995 as a prescription-only product, cetirizine transitioned to over-the-counter status in 2007, underscoring its well-established safety and tolerability profile.
It is derived from hydroxyzine, a first-generation antihistamine, but unlike its predecessor, cetirizine exhibits limited penetration across the blood-brain barrier. This pharmacokinetic property substantially reduces sedation risk, a common drawback of earlier antihistamines.[1]
Pharmacological Class: Antihistamine
(a) Seasonal allergic rhinitis (SAR)
Cetirizine is indicated for mitigating symptoms linked with SAR in adults and kids aged 2 years and older. It effectively alleviates sneezing, runny nose, nasal itching, and eye-related symptoms such as itching, watering, and redness, commonly triggered by outdoor allergens like pollen from trees, grasses, and weeds.
(b) Perennial allergic rhinitis (PAR)
Cetirizine is approved for the management of PAR in adults and children as young as 6 months. It provides relief from symptoms elicited by year-round indoor allergens—such as dust mites, pet dander, and mold—including sneezing, nasal discharge, postnasal drip, nasal itching, and itchy, watery eyes.
(c) Chronic idiopathic urticaria
Cetirizine is indicated for easing chronic idiopathic urticaria in adults and children aged 6 months and above. It markedly reduces itching and helps control the appearance, severity, and duration of hives, offering effective care of this recurring skin ailment. [2]
(d) Allergic conjunctivitis
Cetirizine's ophthalmic formulation is FDA-approved to manage allergic conjunctivitis. [1]
Cetirizine is a rapidly acting, highly selective blocker of the peripheral histamine H1 receptors. These receptors, which cetirizine targets, are primarily located on the smooth muscles of the respiratory system, vascular endothelial cells, immune cells, and within the gastrointestinal tract. Unlike first-generation antihistamines like doxylamine and diphenhydramine, cetirizine has a limited ability to penetrate the blood-brain barrier. This results in minimal interaction with CNS neurons. Consequently, it causes considerably less drowsiness than earlier antihistamines.
By blocking H1 receptors, cetirizine counteracts many histamine-mediated responses. Similar to other second-generation antihistamines, it decreases capillary permeability, thereby limiting fluid leakage into surrounding tissues. Additionally, it is beneficial in preventing bronchospasm triggered by histamine. Moreover, cetirizine exhibits notable anti-inflammatory effects. It has been shown to lower the accumulation of inflammatory cells in ailments such as allergic rhinitis. In particular, it limits the migration of neutrophils and eosinophils (key players in allergic inflammation). [1]
Dosage forms & strengths
General adult dose (Allergies/Urticaria):
Dosing in renal impairment (Oral):
Dosing in hepatic impairment:
Absorption
Cetirizine is promptly absorbed following oral administration, with peak plasma levels (Tmax) typically reached within approximately 1 hour when taken as either tablets or syrup in adult subjects. Its bioavailability is comparable between these two formulations. In a study involving healthy adults who received 10 mg tablets once daily for 10 consecutive days, the average maximum plasma concentration (Cmax) was reported to be 311 ng/mL.
Although food intake does not markedly affect the overall cetirizine exposure (area under the curve [AUC]), it does delay the time to peak concentration (Tmax) by about 1.7 hours and decreases the peak concentration (Cmax) by approximately 23% when taken with food.
Volume of distribution
Cetirizine distributes moderately within the body, with an apparent volume of distribution estimated at 0.44 ± 0.19 L/kg. This suggests that the drug remains largely within the bloodstream and extracellular fluids.
Protein binding
The mean plasma protein binding is 93%.
Metabolism
In a clinical mass balance study involving 6 healthy male participants, about 70% of the administered cetirizine-related radioactivity was recovered in the urine, while around 10% was found in the feces. Notably, about half of the radioactivity eliminated in the urine was due to unchanged cetirizine. The rapid rise in plasma radioactivity was mainly attributable to the parent compound, suggesting that cetirizine undergoes minimal first-pass metabolism.
As a result, the likelihood of hepatic cytochrome enzyme-linked drug interactions is low. Cetirizine is only partially metabolized, primarily via oxidative O-dealkylation, forming a metabolite that lacks significant antihistaminic activity. The specific enzymes responsible for this metabolic step remain unidentified.
Route of elimination
Cetirizine is primarily excreted via the kidneys. Following oral administration, 70–85% of the dose is recovered in the urine, while 10–13% is eliminated via feces. Due to its renal route of elimination, dose adjustments are necessary in those with moderate-to-severe renal impairment and in those undergoing hemodialysis.
Half-life and clearance
The plasma elimination half-life is approximately 8.3 hours. Its apparent total body clearance is estimated at around 53 mL/min. [2]
Cetirizine must not be used in individuals with known hypersensitivity to the drug itself or any of its components. It is also contraindicated in patients with a known allergy to hydroxyzine, given that cetirizine is a metabolic derivative of hydroxyzine. [1]
A phase 3 randomized noninferiority trial led by Abella BS et al. evaluated IV cetirizine as an alternative to IV diphenhydramine for acute urticaria in emergency and urgent care settings. Among 262 adult patients, IV cetirizine was found to be noninferior in reducing pruritus at 2 hours and illustrated several advantages: substantially less sedation, fewer anticholinergic side effects, shorter treatment center stays (1.7 vs. 2.1 hours), and fewer return visits (5.5% vs. 14.1%). These findings support IV cetirizine as a safer and more efficient treatment option for acute urticaria. [6]
A systematic review and meta-analysis led by Zhou P et al. investigated 22 randomized or quasi-randomized controlled trials with 5,867 children diagnosed with various allergic diseases, including PAR, SAR, atopic dermatitis, and other allergic conditions. The study assessed cetirizine's efficacy, acceptability, and safety when compared to placebo or other treatments.
Results showed that cetirizine markedly improved allergic symptom scores over 1 to 12 weeks in children with AR (e.g., at 12 weeks: mean difference, -5.63), and also enhanced quality of life (mean difference at 12 weeks: -23.16). Furthermore, it demonstrated similar effectiveness to other antihistamines and montelukast but did not show superiority in mitigating atopic dermatitis symptoms. Safety outcomes indicated that cetirizine was generally well-tolerated without increased risks of severe adverse events, including cardiotoxicity or CNS effects, although it was linked with a higher likelihood of somnolence when compared to placebo (relative risk, 1.62). [7]
Two phase III clinical trials investigated cetirizine ophthalmic solution 0.24% versus vehicle in alleviating allergen-triggered conjunctivitis using the Ora Conjunctival Allergen Challenge (CAC) model. Study 1 was conducted at a single center, while Study 2 involved multiple centers. Study 2 included participants with more severe symptoms. Around 100 subjects were randomized in each study after allergen response screening. The key outcomes assessed were ocular itching and conjunctival redness at 15 minutes and 8 hours after the intervention.
Cetirizine remarkably reduced ocular itching at all measured time points and lowered conjunctival redness at 7 minutes post-CAC, compared to vehicle. Secondary outcomes also showed prominent improvements in chemosis, eyelid swelling, tearing, ciliary and episcleral redness, and nasal symptoms. The effect was more pronounced in Study 2. No safety issues were identified. Overall, cetirizine ophthalmic solution 0.24% illustrated rapid onset (15 minutes), prolonged action (up to 8 hours), and a favorable safety profile in allergic conjunctivitis. [8]












Comments (0)