Categories
Change Password!
Reset Password!


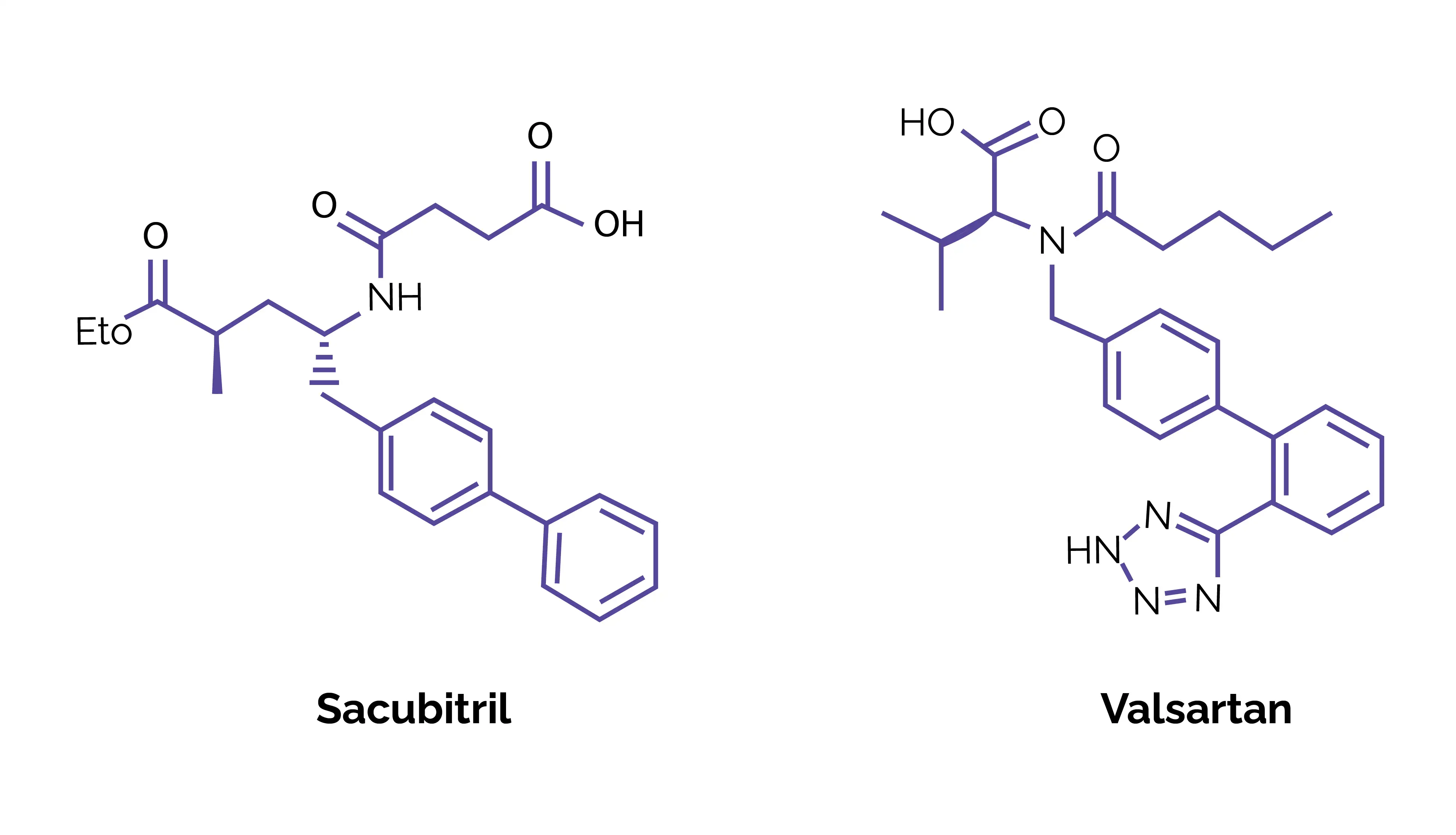
Sacubitril, an FDA-approved neprilysin inhibitor, is used in combination with valsartan for treating chronic heart failure with reduced ejection fraction (HFrEF).
Sacubitril, an FDA-approved neprilysin inhibitor, is used in combination with valsartan for treating chronic heart failure with reduced ejection fraction (HFrEF). It was approved in 2015 under priority review, and marked a pivotal advancement in heart failure (HF) therapy.
By inhibiting neprilysin, sacubitril enhances the levels of beneficial natriuretic peptides, promoting vasodilation, natriuresis, and diuresis. When paired with valsartan, it provides synergistic cardiovascular protection, improving cardiac function and reducing the risk of hospitalization and cardiovascular death.[1]
Pharmacological Class: Angiotensin receptor neprilysin inhibitor (ARNI)[2]
Sacubitril–valsartan therapy is indicated for:
1. Chronic HFrEF
2. Heart Failure with Preserved Ejection Fraction (HFpEF)
3. Pediatric HF
4. Cancer Therapy–Related Cardiac Dysfunction (CTRCD) (Emerging/Investigational Use)
Sacubitril–valsartan exhibits rapid absorption and dual-path activation, designed to optimize cardiovascular efficacy and therapeutic precision.
Absorption
Upon oral administration, the combination swiftly dissociates into sacubitril and valsartan. Sacubitril is rapidly hydrolyzed to its active metabolite LBQ657, achieving ~60% bioavailability. Peak plasma levels occur at 0.5 h (sacubitril), 2 h (LBQ657), and 1.5 h (valsartan). Steady state is attained within 3 days, with negligible accumulation. Food has no significant impact, allowing administration with or without meals.
Distribution
Both agents display broad tissue distribution (103 L for sacubitril, 75 L for valsartan) and high plasma protein binding (94%–97%). LBQ657 shows minimal CNS penetration (~0.28%).
Metabolism
Sacubitril undergoes esterase-mediated hydrolysis to LBQ657, while valsartan experiences limited metabolism (~20%), yielding trace hydroxyl metabolites.
Elimination
Elimination occurs through renal and fecal routes — 52%–68% (as LBQ657) and 13% of valsartan via urine, and 37%–48% (LBQ657) and 86% of valsartan via feces. The mean half-lives are 1.4 h (sacubitril), 11.5 h (LBQ657), and 9.9 h (valsartan). [2]
Sacubitril–valsartan is contraindicated in the following clinical scenarios:
1. Dual Inhibition of the Renin-Angiotensin-Aldosterone System (RAAS)
2. Potassium-Sparing Agents
3. Nonsteroidal Anti-Inflammatory Drugs (NSAIDs), including cyclooxygenase-2 (COX-2) inhibitors
4. Lithium
The most common side effects are:
1. Sacubitril–valsartan has demonstrated remarkable efficacy in improving outcomes for patients with chronic HF. In a pooled analysis of the PARADIGM-HF and PARAGON-HF trials involving 13,194 participants, the drug significantly reduced all-cause hospitalizations compared to standard renin-angiotensin system inhibitors. Over a 2.5-year median follow-up, sacubitril–valsartan achieved an 8% reduction in hospitalization risk (hazard ratio [HR] 0.92; 95% confidence interval [CI] 0.88–0.97; P = .002) and an absolute risk reduction of 2.1 per 100 patient-years. The most pronounced benefits were witnessed in those with LVEF < 60%, reflecting fewer cardiac and pulmonary admissions. Thus, sacubitril–valsartan proved to be a clinically superior therapy that boosts patient outcomes, lowers hospitalization rates, and improves overall HF management.[5]
2. Early initiation of sacubitril/valsartan post–acute myocardial infarction (AMI) delivers remarkable cardioprotective and remodeling benefits compared to conventional therapy. In a study involving 295 AMI patients, treatment with sacubitril/valsartan + standard care produced superior cardiac recovery versus benazepril-based regimens. At 6 months, patients receiving sacubitril/valsartan demonstrated:
These outcomes affirm sacubitril/valsartan’s dual advantage—protecting cardiac function while enhancing ventricular recovery. Early use post-AMI can curb ventricular remodeling, boost myocardial performance, and improve long-term prognosis, making it a cornerstone in modern cardiac therapeutics.[6]
3. A pooled meta-analysis of 14 randomized controlled trials (n = 25,167) reinforced sacubitril/valsartan as a cornerstone therapy in chronic HF, offering superior clinical outcomes compared to traditional ACE inhibitors and ARBs. The key findings were:
Collectively, these findings established sacubitril/valsartan as a clinically validated and mechanistically advanced therapy that improves outcomes in HF.[7]
1. Sacubitril. Drug Bank [DB09292]. Available from: https://go.drugbank.com/drugs/DB09292
2. Nicolas D, Patel P, Reed M. Sacubitril-Valsartan. [Updated 2024 Feb 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507904/. Bookshelf ID: NBK507904, PMID: 29939681.
3. Sacubitril. PubChem [9811834]. Available from: https://pubchem.ncbi.nlm.nih.gov/compound/Sacubitril
4. Sacubitril. FDA Label. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2024/207620s025,218591s000lbl.pdf
5. Lu H, Claggett BL, Packer M, Lam CSP, Swedberg K, Rouleau J et al. Effects of Sacubitril/Valsartan on All-Cause Hospitalizations in Heart Failure: Post Hoc Analysis of the PARADIGM-HF and PARAGON-HF Randomized Clinical Trials. JAMA Cardiology. 2024 Nov 1;9(11):1047-1052.
6. Liu Z, Cui K, Wang G, Jin W, Yao Q, Zhang Y. A clinical randomized trial: Effects of early application of sacubitril/valsartan on ventricular remodeling and prognosis in acute myocardial infarction patients. Contemporary Clinical Trials Communications. 2024 Jul 25;42:101303.
7. Evbayekha E, Idowu AB, LaRue S. Sacubitril/Valsartan vs ACE Inhibitors or ARBs: A Systematic Review and Meta-Analysis of Randomized Trials. JACC: Advances. 2025 Mar;4(3):101598.












Comments (0)